
Food allergies and economic development Are they linked?
This article investigates the impacts of economic transition on global health, with a focus on the increase of food allergies in newly emerging economies

Allergies are commonly perceived as a ‘disease of affluence’ and are thought to be rare in the developing world. Certainly, recent decades have witnessed the emergence of a food allergy epidemic across the developed world, in North America, Australia and Western Europe. However, data now show that the high-income urban centres in Africa and South America are starting to mirror Europe in allergy prevalence. Indeed, in countries such as Egypt, Nigeria and Ghana rates of allergy range between 20% to 30%, matching the morbidity of HIV/AIDS and malaria (Hossny 2019).
This rise may simply reflect previous underreporting and under-diagnosis as well as issues limiting in-country research. (Note the large data gaps shown in Figure 1.) However, it also reveals parallels with human development, adoption of ‘Western lifestyles’, cultural diffusion and the impacts of globalisation and transnational corporations (TNCs).
The World Health Organization in 2000 described some of the largest killers in highincome countries as heart disease, diabetes and dementia. This was in stark contrast to leading causes of fatality in some low-income countries (LICs): malnutrition, malaria, tuberculosis and HIV. Following significant economic transition, the balance is now tipping and Dr George Attim says there are ‘more similarities than differences’. In terms of the dramatic rise in allergy diagnosis, the award-winning study by Yehia M. El-Gamal (2017) states ‘there is now an allergy epidemic in Africa, and not enough specialists to deal with it’.
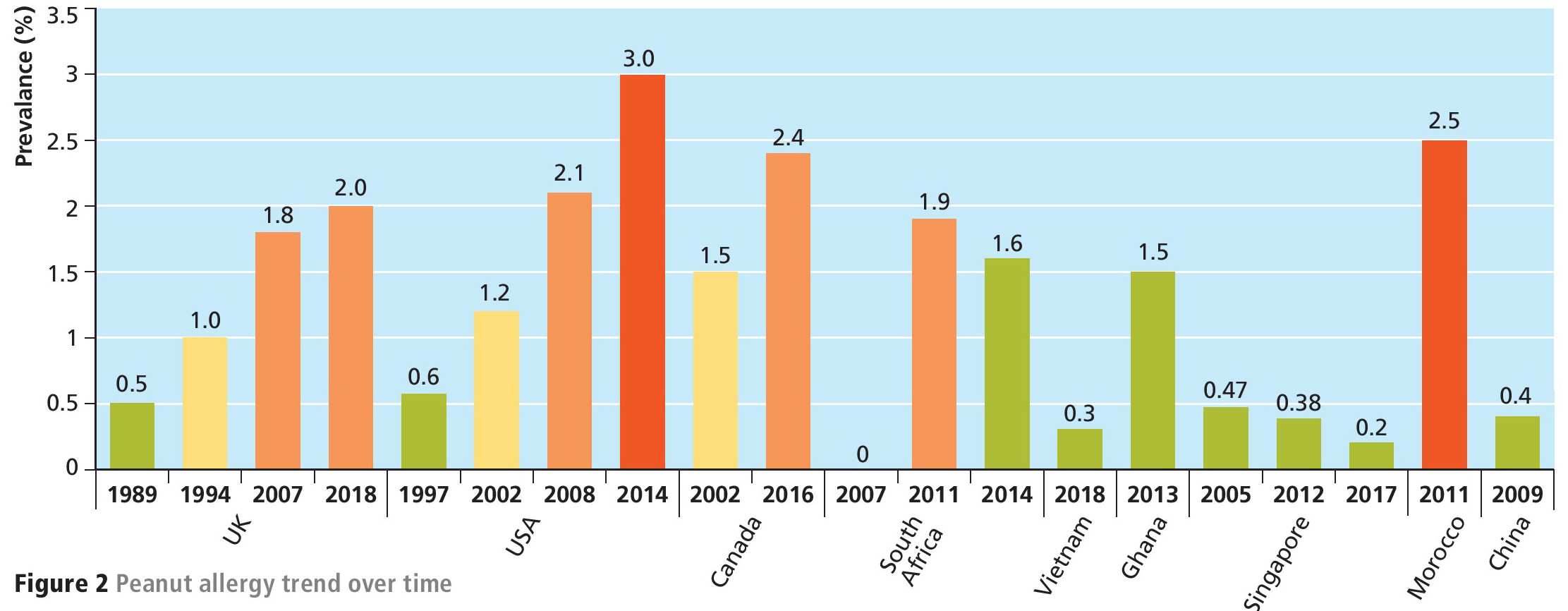
Though there is a clear correlation between economic transition and the prevalence of allergies, finding the underlying causes is difficult. Expert Elham Hossney describes the ongoing problems of data collection, unreliable data and health infrastructure variations between countries. This means cause and effect cannot currently be established. That said, there is compelling evidence of a rise in allergy (see Figure 2) and of allergy prevalence appearing in newly emerging economies. Dr Alexandra Santos explains how this allergy rise is often blamed on changes in diets, vitamin D deficiency, the market dominance of TNCs and urban lifestyles. In some cases, these hypotheses rival, and even contradict, each other.
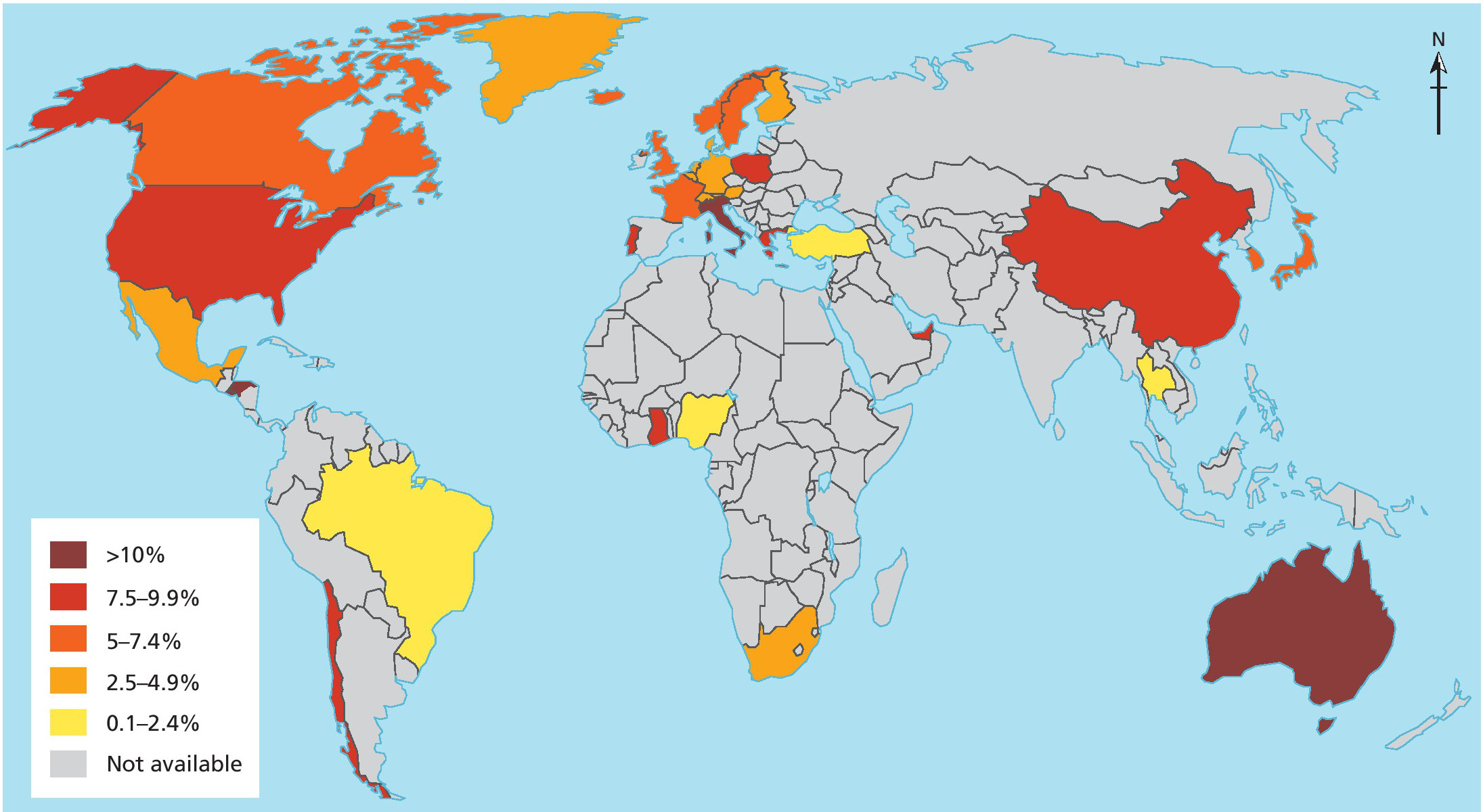
Note: Available estimates of paediatric food allergy around the world varying in food allergy measurements and paediatric groups. Most studies only studied children under 5 years old Source: Center for Food Allergy and Asthma Research (CFAAR)
Allergy on the rise
Over the past 30 years, Britain has seen a threefold increase in the number of individuals with a peanut allergy. And in the last decade there has been a 615% rise in hospital admissions for anaphylaxis, a lifethreatening condition where allergy sufferers’ immune systems release chemicals that flood the body during a reaction. It is currently estimated that globally, between 20% to 40% of the world’s population have at least one allergic condition, with food allergies standing at 8% in the USA, 9% in Australia and 7.5% in Canada (Santos 2018). Box 1 shows the most common food allergies globally.
In the developing world, meanwhile, the trend is similar, although studies are less common. In a 2007 South African study, Professor George Du Toit’s trial results showed zero proven peanut allergy. Seven years later the allergy to peanuts increased to 1.6% (Basera 2015).
Box 1 Top eight food allergies for under 18s globally
■ Europe — Dairy/Fish
■ North America — Shellfish
■ South America — Soy
■ Asia — Wheat
■ Africa — Tree nut
■ Oceania — Egg
Source: ESPEN Congress Krakow 2019 Digestive Allergies and Intolerances


In China, some like to chart the rise from 1990s, the emblematic decade when the fastfood chain McDonald’s opened its first outlets. In the city of Chongquin the prevalence of food sensitisation and allergy in children climbed from 9.9% to 18%, coincidently following the first McDonald’s opening in 1999. Interestingly, McDonald’s outlets have now become so ubiquitous around the world as globalisation proceeds, that The Economist magazine uses the cost of the renowned ‘Big Mac’ as a comparison point for cost of living (The Big Max Index).
Food and Foreign Direct Investment
Globalisation, a term coined in the 1960s, is the increasing interconnectedness and interdependence of the world economically, culturally and politically. The phenomenon led to an increasing volume of cross-border transactions in goods and services, freer international trade and a rapid diffusion of ideas and technology. Health, too, is increasingly perceived as the integrated outcome of environment, social-cultural and economic factors.
In the case of allergies, one can see how food is consumed with spatial and temporal variations and with differing equalities. Dr Cheng S. Wang (2018) discusses how heavily processed foods, and the introduction of untraditional food stuffs, may have profound impacts on health and increased risk of asthma and allergic diseases.
TNCs such as McDonald’s and Yum! Brands (owner of KFC and Pizza Hut) input Foreign Direct Investment (FDI) cash and locate branches in new and developing markets. Customers’ everyday diets shift swiftly. ‘McDonaldisation’ and ‘CocaColarisation’ became buzzwords as brands moved into poorer countries’ markets, and rapidly became associated with modernity and desirability. International chains also tailor their products to local tastes, dubbed ‘glocalisation’, boosting demand. In Nigeria, Domino’s Pizza and KFC sell jollof rice dishes, a West African staple.
Many international food chains are under the control of TNC market power. Of the top 100 economic entities in the world, 69 are corporations while just 31 are countries (Action Aid). Global food processors and providers are among the big names, including Walmart, Nestlé, Kraft Foods, Unilever, PepsiCo, and are very influential. In Ghana, for example, obesity rates have grown by more than 650% since 1980, when KFC first became established as a status symbol (NY Times 2017).
Dr Wang and other researchers state it is unclear what makes fast-food products potentially responsible for the rise in food allergies, but high saturated-fat content may have a role — this causes the production of inflammatory cells and can also deliver poorer levels of nutrition. Antibiotics and chemicals used in fast-food may also reduce the body’s exposure to important microbes which help prevent allergy development in children.
Sunshine and urbanisation
Other powerful causes may be equally important. Economic growth in developing countries can be expected to result in improved standards of living and human development, with improved sanitation, increased life expectancy and literacy rates. Along with this comes a shift from agricultural, primary-sector jobs, into secondary-and tertiary-sector employment. As incomes rise, citizens increasingly work long hours indoors, reducing the levels of the vitamin D received (the sunshine vitamin), and time pressures lead to a desire for eating out, pre-packaged and processed food.
Dr Eyal Oren (2008) compiled studies and found an increased likelihood of potential for allergy in obese patients with vitamin D deficiency. Regions in low latitudes (and therefore with high insolation) are also correlated with lower allergy rates says Dr Alexandra Santos (2020). Patterns can be seen revealing that closer to the equator, across southern USA and northern Australia, EpiPen prescriptions are the lowest (EpiPens are devices that deliver an adrenaline shot during anaphylaxis) (Camargo 2007 and Mullins 2009).
Economic shifts also tie in with urbanisation. Over 55% of the global population lives in a city and the most rapid urbanisation of megacities is projected to be in Africa, Asia and South America. Rapidly urbanised areas are associated with higher levels of sanitation, hygiene and access to medical care, which have greatly improved quality of life and health. Urbanisation also includes higher rates of pollution and respiratory disease like asthma. Higher hygiene levels combined with air pollution are both factors hypothesised to currently be causing food allergy in the developed world.
Box 2 Links to geographical skills
Research and studies in allergies are difficult to compare and involve a number of extraneous (uncontrollable) variables and must therefore be used with some degree of caution. Qualitative (opinion-based) data from questionnaires and self-reporting help generate a hypothesis and provide case-specific accounts. This qualitative data often use small sample sizes and are subjective. Quantitative (numerical) data from allergy testing are more objective and comparable but cannot always be extrapolated (generalised to other contexts).
The winners and losers
Big pharmaceutical firms spend huge amounts on advertising and make vast profits. This may encourage people to believe they need to take drugs that can often be unnecessary. In the USA, for example, approximately 20–25% of adults believe they or their children are afflicted with a food allergy and alter their diets unnecessarily. An EpiPen pack currently costs £89.99 (Lloyds Pharmacy 2020) and so, regardless of whether allergies are increasing or simply being newly reported, the most underprivileged members of society worldwide will be financially excluded from accessing such drugs.
Case study: South Africa
Traditionally, South Africans have enjoyed low rates of food allergy and those of black descent were thought to be protected against the allergy epidemic. South Africa was the first African nation to become a newly emerging economy (NEE) and now has the second highest GDP in Africa. South Africa provides a useful case study to explore the impacts of economic development, rapid urbanisation and food allergy as research and data in the country is the most robust on the continent.
Recent decades have been labelled the ‘second wave’ of allergy, witnessing a rise in evidence for food allergy in South Africa. Currently, food allergy is diagnosed in 2.5% of Cape Town’s children and up to 40% in those predisposed to allergy (those with eczema). Dr Claudia Gray (2012) states that as indigenous populations urbanise and take on ‘Westernised’ lifestyles and diet, this could impact food allergy and become a major health burden.
Income and urbanisation
The economic transition in South Africa has led to significant industrial structure change. The government is campaigning to attract $100 billion of FDI by 2023 and agriculture
makes up just 2.8% of the economy. South Africa has the largest foodservice market in sub-Saharan Africa and the growing middle class are increasingly spending money on food higher in fats and sugars. Almost 70% of South African women and 31% of men are overweight or obese. Furthermore, the Malabo Montpellier Panel (MMP) report that processed foods account for 70–80% of the middle class’s food budget. The easy availability of fast-food products is anticipated to impact cooking practices — that is, decreasing the frequency of home cooking and creating a dependency on processed foods.
Second, over 65% of the South African population is urban. This rural-to-urban migration means people experience new environments and lifestyles. In the USA, nearly 10% of children in cities have a food allergy compared to 6.2% in rural areas. The results of a Cape Town study suggest that food allergy is also now comparable to the industrialised middle-income countries — 9% in urban populations compared to 2.8% in rural. Santos (2018) studied allergy in immigrants in the UK and also found that migrants can develop allergies in new settings.
Poverty and protection
Quality of life and inequality in cities could be a contributing factor. South Africa’s Human Development Index (HDI) is high: 0.705. However, inequality is rife, with a Gini Index placing it as the most unequal of African nations. South Africa is plagued by a rich– poor divide, as well as sanitation and housing problems, with 23% of the population living in slums. In line with a hygiene hypothesis, this should in fact help protect poorer populations against allergic conditions.
Lastly, race in South Africa defines its history, politics and balance of equality. Allergy studies have found that for black South African children (Xhosa) there is a lower prevalence of peanut allergy than in mixed-race Caucasian/black children. Moreover, in 2014, peanut allergy was just 15% in black Africans and up to 38% in other ethnic groups. The risk of developing food allergy was, however, higher for children of African ancestry born in developed countries compared to children of Caucasian ancestry.
Conclusion
Global development and its economic successes come with many negative implications for the environment, such as pollution, deforestation, species decline and climate change. However, the Sustainable Development Goals have helped improve human development indexes, and economic transition of countries such as the BRICs (Brazil, Russia, India, China) and MINTs (Mexico, Indonesia, Nigeria, Turkey) have seen great rises of GDP and HDI. Many have now hypothesised how these shifts may also be amplifying allergy in developing and middle-income countries like South Africa.
There are various attempts to unpick the link. Explanations such as the hygiene hypothesis, vitamin D deficiency and diet are at the forefront of most studies. The shift towards urbanised lifestyles, reduced microbial exposures, indoor jobs and less home cooking are all likely to be to blame. The understanding of causes of allergy are still limited and reliable data is lacking, particularly in sub-Saharan Africa. In countries such as South Africa where the number of doctors per 1,000 people is only 0.910 or Nigeria at 0.383 (the UK is 2.8), it is important we gain a better understanding of allergies globally, and the potential consequences of rapid urbanisation and development on these lifethreating conditions.
Questions for discussion
1 Do you eat fast food? What makes it desirable?
2 What factors might make foreign direct investment difficult for TNCs?
FURTHER READING
Santos, A. (13 September 2019) ‘Why the world is becoming more allergic to food’, BBC News: www.tinyurl.com/y5567nnj.
Allergy UK national charity: www.allergyuk.org.
World Bank in South Africa: www.tinyurl.com/y36s9uhr.
KEY POINTS
■ Allergies are usually seen as a highincome country (HIC) disease.
■ Economic development has been hypothesised to lead to increased food allergy in developing nations.
■ Allergy prevalence in Africa now ranges between 20–30%, suggesting a morbid condition matching HIV/AIDS and malaria.
■ Fast-food consumption, sunshine deficiencies and urban living are potentially to blame for the allergy rise.
■ South Africa has seen a rise in reported allergies, particularly in Cape Town.